

Maybe we should write an obituary for the website

It’s time to hold a funeral for healthcare websites as we know them.
This week, Google announced an update to AI Overviews that is going to continue to send health system websites (as we know them) to the grave. I know this because, following the announcement, I did a little research project and the results were quite interesting.
But, first… let’s review what Google announced.
Every year, during The Checkup, Google announces how it is bringing “the best of Google to the world of health” and this year their announcement regarding health searches didn’t seem to be that big of a deal, unless you really sit and think about it.
Google announced that they are providing “helpful health results in search” by increasing the number of AI Overviews they will show for healthcare queries to “cover thousands more healthcare topics” and will do so in additional languages besides English. They are also helping people essentially “crowd source” information through an addition to the results called “What People Suggest.”
On first glance, this isn’t really that big of a deal. On face, I’d say, “Ok, so Google is going to add more AI Overviews to give people quicker healthcare answers. Great!”
But if you dig into this a bit, this is actually a pretty huge deal. Here are some stats to consider:
1 Billion people worldwide are exposed to AI Overviews every month.
As of February 2025, Google’s global search market share is 90.15%. This means people are still going to Google to find information (even with other platforms trying to steal share).
In 2019, Google said approximately 7% of healthcare searches happen every day. That’s 70,000 healthcare searches per minute. (That was 2019, so I’d imagine it’s even larger now.)
As of June 2024, 63% of results for a healthcare query showed an AI overview. AI Overviews are showing for healthcare more than any other industry.
Organic click-through-rates decline 70% when an AI Overview is present. That means more than ⅔ of people are not clicking through to a website if they are getting the summary via an AI Overview.
Even without this week’s Google announcement, this data is pretty damning for healthcare websites and anyone with a content strategy to ensure health system content and individual pages have any chance at appearing when someone is searching for a provider or researching a condition or procedure. Google’s introduction of SGE-now-named-AI Overviews turned SEO on its head and traffic to websites has not recovered. (Remember when I mentioned the Chegg lawsuit in last week’s newsletter?)
For the last few weeks, I’ve been writing about how AI and different technologies are going to change how people interact with platforms to find information about healthcare. But Google still dominates where people are finding health information, so I thought this announcement needed some attention in this week’s newsletter, because of the implications of increasing the number of AI Overviews they plan to show for healthcare queries, specifically.
Following The Checkup announcement, I decided to do a little analysis of my own to see what kind of impact AI Overviews and improved Symptom Cards might be on a website in my local market – MassGeneral Hospital (www.massgeneral.org). This is not a scientific study, but I hope it illustrates the points I’ve been making over the last year. (And not to single out MGH, but Beth Israel Lahey Health and Tufts Medicine both didn’t have content pages that I could easily find on their sites, so I opted to run this experiment with the only site that did — MassGeneral’s site).
Here is what I did:
I went to MGH’s website and clicked on the “conditions and treatments” section, and clicked conditions A-Z.
I wanted to see whether the condition pages on MGH’s website showed up on Google when I searched for a condition, so I clicked on each letter and found the first condition listed, searched for it and recorded it if it had a Symptom Card on Google. If it didn’t have a Symptom Card, I searched for the next condition in that letter. (I ended up with 24 conditions because Q and X didn’t have listed conditions on MGH’s site.)
I added the condition to the first tab (“Condition”) on this spreadsheet, along with the URL of the search result.
I reviewed each Search Engine Results Page (SERP) and documented which organizations appeared for each condition. I listed “y” if the site was included in the results.
On the second tab (“Who is the best…”) of the spreadsheet, I did a basic search for “who is the best provider for ____” for each condition and repeated my steps, as above.
My goal was to see if MGH's condition pages from its website showed up for any of these searches. After all, every condition I searched for had a corresponding page on MGH’s website, so it would be safe to assume that MGH should be part of the consideration set if I’m searching for healthcare from a location near MGH (I live 15 minutes away from MGH and I know my IP address is based in “Boston”).
Here’s the shocking reality: For the 24 conditions that I found on MGH’s website, 0% showed up as a result when I searched for the condition on Google. ZERO.
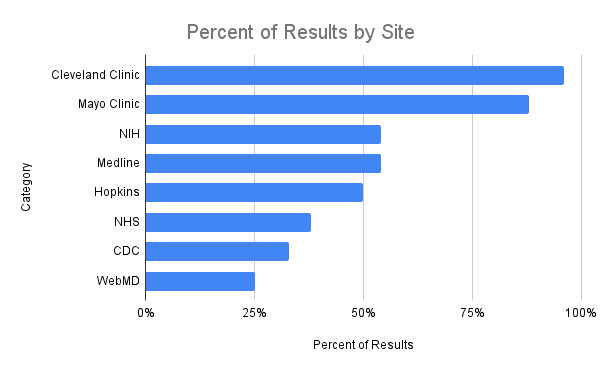
What did I find instead?
96% of the results showed Cleveland Clinic content
88% of the results showed Mayo Clinic content
54% of the results showed NIH content
54% of the results showed MedlinePlus content
50% of the results showed Johns Hopkins Medicine content
For the 24 “Who is the best…” queries, my results were a little more varied. MassGeneralBrigham (“MGB” - I combined MGH, Brigham & Women’s and McLean Hospital results) actually showed 50% of the time). But these results were also curious!
79% of the results showed Mayo Clinic
75% of the results showed discussion sites (Reddit, Quora, etc.)
67% of the results showed condition organizations (e.g., Myocarditis Foundation)
50% of the results showed an MGB organization website
42% of the results showed a local practice or physician group site

So what do we make of this?
My initial reaction is to gasp, and then get to work. I know my “research project” was non-scientific, but here’s what I gleaned from it anyway:
Most people will find the health information they need from three healthcare sites feeding Google’s AI Overviews: Cleveland Clinic, Mayo Clinic and Johns Hopkins Medicine. All of that time, energy and effort spent to go deep on content on a website is all but wiped away given Google’s latest announcement. AI Overviews and Symptom Cards are predominantly sourcing information from these three sites plus a host of government websites. It seems like there is a rare chance that a local organization’s content will surface when someone searches for healthcare. Google mentioned this during The Checkup - they plan to make health information “credible, accessible and easy to understand.” They know that the content they get from the sites they are currently sourcing check all three of those boxes. I don’t anticipate they will change how other content surfaces in the future.
Prioritizing “discussion sites” and crowd sourcing will be create headaches for healthcare organizations. Three-quarters (75%) of all results showed a “discussion site” category, meaning that Google is prioritizing crowd-sourced information and experiences three out of four times someone searches for something health-related. This crowd-sourcing of information means we might be dealing with the wild west for a long time. While Reddit and others are “friendly” sites with moderators, have you even thought about how you might control what people are saying and whether they are recommending the right course of action, procedures, etc., for conditions, procedures, doctors? Now you have to manage comments on these sites in addition to reviews and reputation on third party sites? It seems like this might need to be an additional piece of management that no technology company (that I’m aware of) can yet help control (like they might do with managing online reviews, for instance).
It’s clear that healthcare publishers are toast. When it comes to condition searches, Healthgrades, WebMD, etc. are literally nowhere to be found now that Google is prioritizing additional AI Overviews and Symptom Card results. It doesn’t even seem like Google is sourcing their content from these healthcare-specific sites. So it begs the question: why would you need to rely on sending any data to them if traffic is going to be so diminished in the future? Let’s say you’re employing a listings strategy today: you probably don’t need to worry about sending your data to sites except for the big four (Google, Bing, Facebook, Apple).
Assume that a patient’s first exposure to learning about a health condition or procedure will be covered in an AI Overview and Symptom Card from the big three: Cleveland Clinic, Mayo Clinic and Johns Hopkins Medicine and at least one government site. If a patient wants to dig deeper, assume the patient will opt for a conversational platform (Google’s AI Mode, ChatGPT search, Gemini, Perplexity or others) to learn more. Do not assume that patient will go to your website. Assume, instead, that there is a real possibility that a patient may never reach your site through a SERP click-through any more.
“Big-B” brand-building may end up taking greater mind-share within (what’s left of) marketing teams. Digital competition is changing as SEO changes. If the “big three” healthcare organizations are feeding content to supply AI Overviews with the right information, it means the only way to drive someone to your website will be through brand affinity and recognition. Your website will need to facilitate conversions, so you need to ensure a patient know you exist and can navigate there directly. A few weeks ago, I wrote about agents, so it’s highly likely that patients may never navigate to your site anymore because the agents will do all of the work on their behalf, too.
We are at a point of no return.
I reckon websites need to serve a very different purpose today than they did a year ago. My little non-scientific research project proved my point – websites as “online brochures” with pages and pages of content are dead (or, if not dead, are at least dying). Instead, I’ve recently been thinking about websites as “apps”, meaning, a website needs to serve two purposes, similar to the purposes apps serve on a mobile device:
Help a patient (or an agent) take an action to convert in some way (as in, sign up for a newsletter, find a provider and/or book an appointment); and,
Ensure a patient can perform a non-conversion action, e.g., logging in to do “admin” tasks – see lab results, pay a bill, etc.
Content as an SEO driver to a website will become far less important (it will only be important to the “big three”). If you aren’t the “big three”, assume that people might come to your site to take an action, but largely won’t visit your site as a referral from Google, and that they’ve probably already gotten the information they need before reaching your site. The only reason they will land on your site is to convert. This is how apps work today: I don’t use my Patient Gateway app for MGH or my OneMedical app to do health research. I use it to take an action or convert - to interact with a doctor or book an appointment. So now the website needs to serve that same purpose.
And it also means that – oh, here’s that word again! – DATA becomes the foundation of your online strategy.
Not only do you need to have a command over the data you need to share with platforms that are increasingly taking traffic away from your site, but also what additional data you need to turn your website into a conversion “app” engine. Instead of thinking about name, address, phone number for providers, for example, you need to start thinking more broadly::
Providers, their availability, empty slots, insurance they accept;
Workable online appointment scheduling capabilities, including availability as well as actual working online appointment scheduling tech;
Provider transparency data to help people review, evaluate and select providers;
Quality and outcomes data to present the right provider (rather than the most popular provider) to the patient. For example, you should have data about who is the expert on knee replacements because you know which orthopedic surgeons have billed for more knee surgeries than anyone else — and maybe even quality data associated with those surgeries, too); and more.
I’ve recently talked to a number of healthcare provider organizations who are beginning to explore yet another “website redesign” project, and I’ve talked to a number of technology organizations who are building tools for healthcare websites. I implore everyone to consider what a radical step you need to take to either create the website of the future (that doesn’t include content for SEO purposes but does prioritize conversion opportunities) and/or take a platform-first approach to ensuring your data (and I mean all data) is organized in such a way that you can control when and where information surfaces on any platform and not worry as much about dealing with the traditional concept of the website as it stands today.
I know, it's crazy to think about a world where websites disappear. But let’s face it. That world is right around the corner.
Let’s bow our heads and take a moment of silence of the death of the healthcare website.
Excellent analysis - thank you.
Very impressive Carrie. For healthcare marketers the future has arrived.